David Shifrin: Welcome to DigitaLee, the podcast for healthcare marketers, where we look at the digital news, tools, tips and tricks for effective healthcare communications. I’m David Shifrin with Jarrard Phillips Cate & Hancock, and I’m with Lee Aase, digital healthcare pioneer and now healthcare entrepreneur. Today, we’re looking at the Spanish language misinformation crisis, Meta / Facebook’s recent dive and Apple privacy rules.
So for the first section, I wanted to talk about, we’re back to talking about misinformation in the news. This one is a little bit different. A story on Axios about Spanish language misinformation crisis, and I think everybody’s pretty aware of what’s going on. As far as misinformation, it’s not quite as hot of a topic as it was a few months ago at the peak of the vaccine push, but certainly is still an issue.
And I thought that sort of the core point, the thing that really stood out to me in this article, was between the lines and says where platforms are quick to remove misinformation posts in English, some identical posts in Spanish remain online. And just something that I hadn’t really considered is the multi-lingual nature of everything that’s going on and the need to reach out to so many different communities.
What’s your gut when you see this article?
Lee Aase: I have a little bit of a different take and I thought it was actually a good launching pad to be able to talk about some of this. So I think there is a crisis. I don’t think it’s a Spanish language information crisis, and I think it’s a different one. And we’ll get to that in a little bit.
When I started advocating for social media use by hospitals about 15 years ago now, there were definitely a lot of people interested and then I got a lot of objections because people are saying “what about all the bad information on the internet?”
And my response was, there will always be bad information on the internet. That’s just the way it is. If you have a free and open internet, you’re going to have people publishing bad information. So my answer was then if responsible medical professionals don’t engage, we’re ceding the territory to the snake oil salesman and to the people, the charlatans, the people who are putting out bad information.
And so that’s why I was arguing that health professionals had a moral responsibility to put out good information. I have a good friend of mine that a lot of folks listening to this will probably know. Andy was the founder of the Word of Mouth Marketing Association, or was the president of that.
Anyway, he founded a group called the Blog Council—now that’s socialmedia.org what it later became—anyway, he had a saying that he said he learned in high school chemistry that the solution to pollution is dilution. You know, that if there’s bad stuff out there, you need to overwhelm it with the good, okay. You need to put out reliable, trustworthy information. And the way that we have thought about it for 15 years in social media is that the good information will drive out the bad, the good information that people like it, they’ll comment it, it’ll get up-ranked. There’s a thing on Twitter called the ratio. The ratio is comments versus retweets or likes, and if your comments are much higher, that’s meaning that people are taking issue with what you’re saying versus what, versus liking it or passing it along.
There’s a quote that’s been attributed to Voltaire: “I may disagree with what you’re saying, but I’ll defend to the death your right to do it.” We’re a long way from that right now. You know, we’re saying, yeah, we need to tamp down, we need to drive out this information.
I think that’s a big part of the problem for the polarization that we have now, is that it is viewpoint discrimination and that opinions that align with the governmental or large entity positions are…are those that are aligned are promoted and others are suppressed.
So, over the last several months, users have been banned from Twitter for messages that today we know are true. Cloth masks don’t work. Posting that previously would get you, could get you banned from Twitter. And if the goal is to prevent respiratory infections, they don’t work.
Okay. Cloth masks don’t work. And they’re saying, ‘No, yeah you got to wear N-95s or KN-95s.’ You know, some messages that previously came from government or medical authorities have been shown not to be true. Okay, Israel has a vaccination rate of about 95% for those who are over 50 and about 85% have gotten the booster, and as of February 3rd COVID deaths were at an all-time high in Israel, okay.
The president of the United States, the current one, not the previous one, the head of the CDC and a whole bunch of others have previously said, and the tweets are still up, if you get vaccinated, you won’t catch COVID and you won’t spread COVID. And there aren’t any warning labels on those. There aren’t any things saying this may contain misinformation.
So I think those messages are still up, and I think another issue in addition to this alleged Spanish misinformation crisis is if you can’t be heard on the normal platforms where everybody’s speaking, well, if you park your truck on a bridge and don’t move it, and it’s a bridge between two countries, people are gonna pay attention. They’re gonna listen.
David Shifrin: Going to get noticed.
So I think the fact that things are being suppressed, pushing down on that is kind of why we get, and I know in another…in a future segment, we’ll get into talking about some of these other platforms, GETTR or Parlor and others, but the reason those spring up is because the more mainstream platforms are suppressing it. And I think it’s…so that’s where the problem that I see is the credibility. You know, even if you think it’s harmful, then you should speak out against it instead of banning it, instead of banning individuals and banning and putting labels on that feel like they’re putting the finger on the scale.
So that probably wasn’t what you were expecting when you proposed the top.
David Shifrin: But it’s a good note too, that we have to engage. And to do… and this is something that I’ve been really concerned about for a long time, I’m a scientist by training and we need to do a better job of communicating how science works and how the data is collected and how we analyze it, because it does change.
And that doesn’t mean anybody’s being disingenuous or trying to play rope-a-dope or whatever, but it’s just, this is how science works. It’s complicated and it’s hard. And so the guidance will change. And that should be the message. And that gets to your point about diluting the bad information and just being more clear and straightforward about, ‘Here’s where we are today and here’s how we arrived there and this may change tomorrow.’
Lee Aase: Yeah, science, isn’t a person and it isn’t a noun. The science is a process, it’s a verb, and we need to, yeah, and educating people on the scientific method and what we know because of studies and what they can tell us, and then what the limitations of the studies are. And I realize that you get into a pandemic and people say we gotta get some communication out here because there’s all this bad stuff happening and we gotta give them some clear messages, and they want to give a clear message. And I think the risk of that, and I think what has borne out because of it is that we have people that have much less trust in public health than they would previously.
David Shifrin: Yeah. I love it. Thanks, Lee. Let’s look at the platform of the week. Meta, the artist formerly known as Facebook, the artist formerly known as Mark Zuckerberg’s dorm room. A lot of stories going around recently about how the number of active users has dropped for the first time ever, and as a percentage of total users it’s pretty minuscule, but it did drop.
It’s never happened before. Their earnings are down. Their market cap took a hit largely, or at least in part, because of Apple’s privacy rules, which I think a lot of folks listening as marketers are going to be aware of.
It’s something we’re watching here. So is this a big New York Times headline story that’s a big story because it’s a massive company or is this something that digital marketers in healthcare need to be paying close attention to for potential issues?
Lee Aase: Well, I think marketers should always be paying attention to things like that and be looking at performance. So they need to be looking at what’s really happening in terms of click-throughs and business results that they’re trying to accomplish through it. I think being cognizant, at least of the fact that the user base is diminishing a little bit, or at least the active user base, that paying attention to where the attention of users is going is something that just is basic work that marketers should be doing. Marketers, communicators of all types.
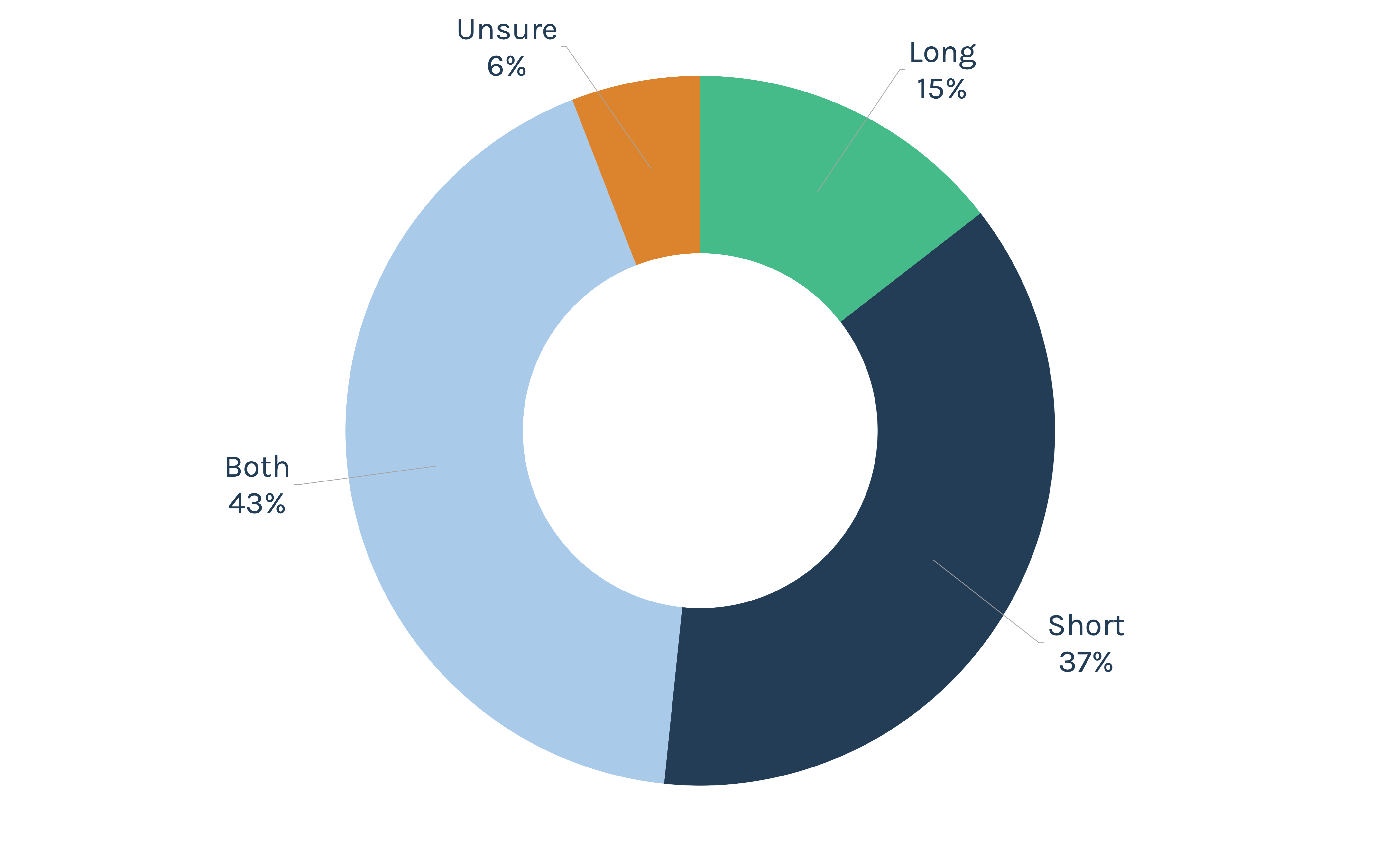
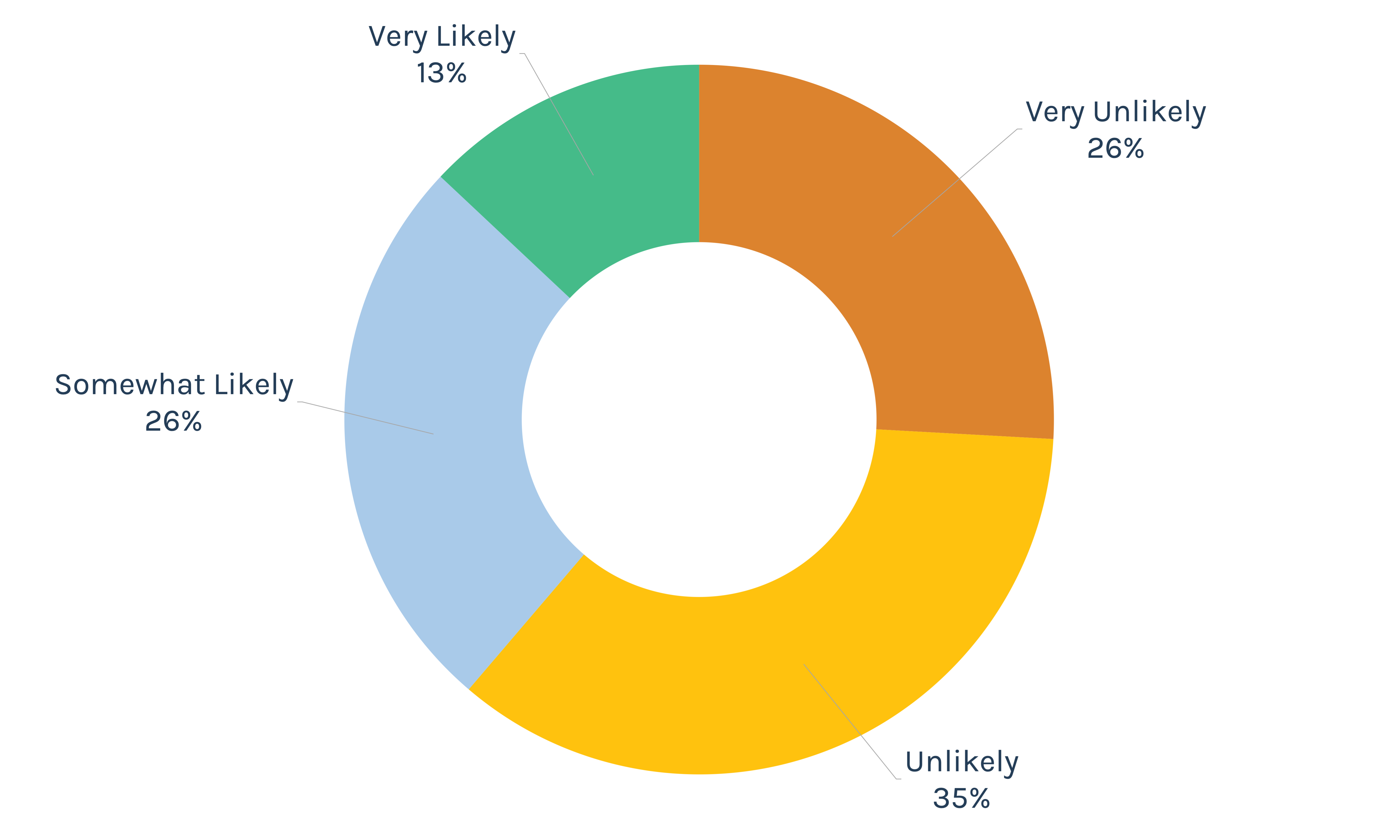
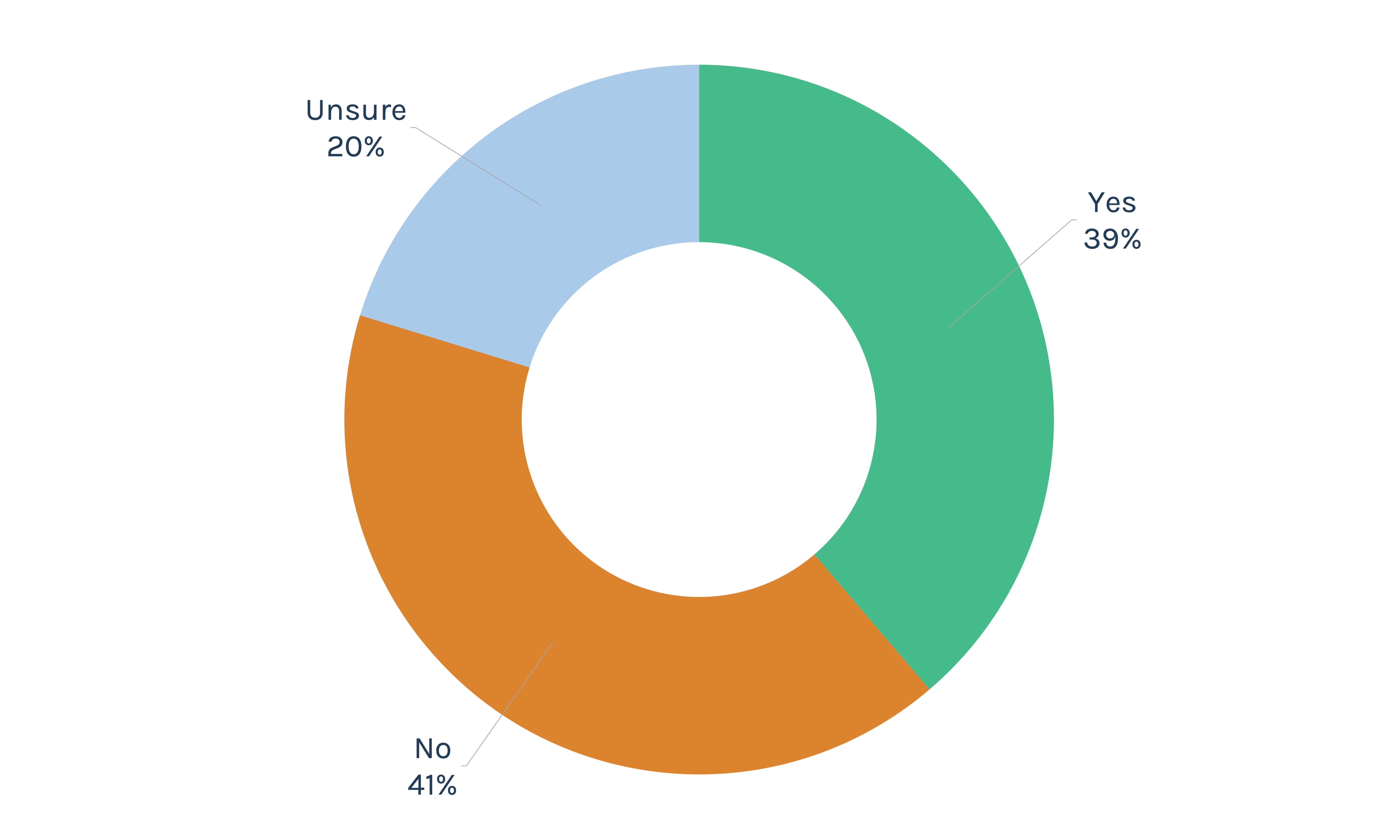
I think that, getting back to the previous issue, we talked about when you have the…I think one of the reasons behind, I mean this is a hypothesis, okay? This is a guess even, you know, that 50%ish, maybe it’s 48% of people and maybe 40% that are pretty strongly feeling that way are saying, you know, this is a platform that’s not friendly to me. Or, that is, this is going to put a label on things that I agree with that says this might be misinformation. I think people then maybe hold back and just say, ‘Okay well, I’ll share my family, kid pictures and watch the grandkids.’
But maybe you’re less likely to…it just takes a little bit of the luster off, I think.
David Shifrin: Yeah. And so then if they’re backing away from their engagement, it’s even harder to reach them, obviously, by definition, with good information. So you’re…
Lee Aase: Right. Yeah. And when you’re…I mean the answer isn’t to turn up the volume, okay. It isn’t to turn up the volume and turn down the screws, it’s to engage and to discuss. And I recognize that having been worked in the healthcare system and where you’re posting the messages that you’re, you know, being given to post, and there are definitely, there are unpleasant conversations that are happening there. The way it is right now, for sure.
David Shifrin: Okay, so let’s keep an eye on it and watch the numbers and see what happens next time Zuckerberg testifies before Congress.
For the last piece here Lee, the tip that I want to focus on is Apple’s privacy rules, which I just mentioned. I think, again, I think a lot of folks are aware of this, but the native iOS Apple mail app, which accounts for a huge chunk of email management, somewhere between 40 and 50-plus percent, it now is pre-loading tracking pixels to obscure human opens and geolocation data.
It’s a privacy push. It reduces the ability for us marketers to track engagement and target across different platforms. And again, this bit into Facebook’s revenue. So it’s potentially a problem for pure marketers selling whatever, clothes or widgets. How much do you think this could matter for the types of campaigns that hospitals and other healthcare providers are running?
Lee Aase: Yeah, well, I mean I think the upshot that HubSpot talked about in that article that we, that I think you referenced and you probably put it in the show notes, is just that marketers need to focus on the harder metrics and the ones that are more business-oriented, like click-throughs, like actual, go to the other one we were talking about here, replies. Yeah.
So, I mean, that’s the thing is when people are actually taking some step, you know, I look at shares for instance as well, shares on social, A share is…I used to call it the mother of all metrics, because it’s not just “I like it,” it’s “I want my friends to see it,” and so those are the things that I am typically going to be paying a bunch more attention to.